Definition
Cardiology is a medical specialty dealing with the diagnosis and treatment of diseases and disorders of the heart.
History
 Cardiology first became a specialized field of study when Jean Baptiste de Sénac in 1749 published a summary of contemporary knowledge of the heart. This was followed 12 years later by Leopold Auenbrugger's discovery that the condition of the heart can be estimated by the sound returned from tapping on the chest (percussion). Listening to heart sounds became a major part of medical diagnosis after René Laënnec's invention of the stethoscope in 1816.
Cardiology first became a specialized field of study when Jean Baptiste de Sénac in 1749 published a summary of contemporary knowledge of the heart. This was followed 12 years later by Leopold Auenbrugger's discovery that the condition of the heart can be estimated by the sound returned from tapping on the chest (percussion). Listening to heart sounds became a major part of medical diagnosis after René Laënnec's invention of the stethoscope in 1816.
Much of the development of cardiology during the 19th century consisted of improved diagnostic methods. An important diagnostic advance was Willem Einthoven's invention in 1903 of the electrocardiograph, which measures the heart's electrical activity; by 1915 the basic methods of diagnosis of heart disease, including fluoroscopic studies of the beating heart, were in place. Various advances in diagnostic technology opened up the possibility of surgical correction of many heart problems.
Cardiology itself remains a medical, not a surgical, specialty although cardiologists work closely with surgeons in cases of heart surgery. Cardiologists provide the continuing care of heart patients, performing basic studies of heart function and supervising all aspects of therapy, including the administration of drugs to modify heart functions.
Much of the development of cardiac medicine in the second half of the 20th century has been in the field of heart surgery. Major advances in this field have included the routine repair of coronary artery disease, one of the major causes of heart attacks; the first human heart transplant, performed by Christiaan Barnard of South Africa in 1967; and the development of a permanently functioning, surgically implanted artificial heart by a research team at the University of Utah, first used in 1982.
Cardiovascular system
History
Description of cardiovascular system
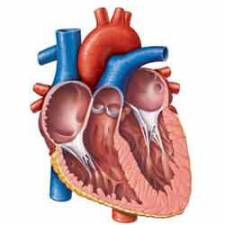
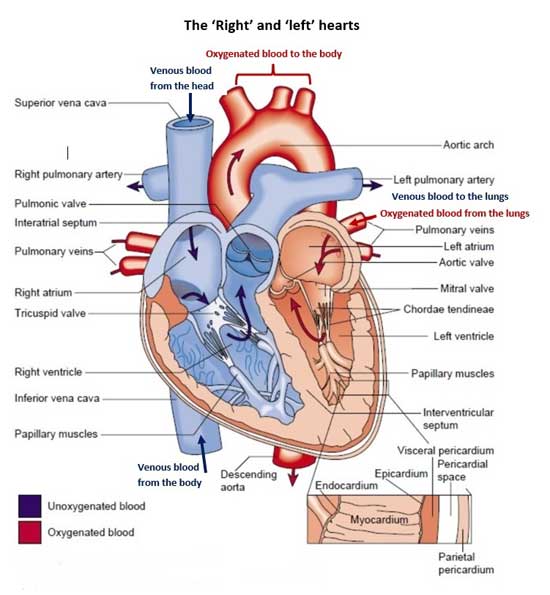
The cardiovascular system consists of the heart, a muscular hydrodynamic pump, and its conduit vessels, the arteries and veins. Through this hydraulic circuit flows blood carrying oxygen and nutrients to all parts of the body, and transporting accumulated toxic metabolites to the kidneys, liver and lungs for elimination. The heart in fact is two pumps, the right and left heart, which are connected in series and which independently circulate blood to the lungs or to the rest of the body, respectively. Each of these pumping systems, right and left, consists of a small, thin walled atrium which collects blood and forces it into a larger thick walled ventricle which generates enough pressure to move the blood to the lungs or the rest of the body. Since the heart muscle alternately contracts to expel blood and relaxes to take in blood, the pressure in arterial conduits varies in a pulsatile fashion.Reflecting this, blood pressure in the body (the left heart or systemic circulation) is measured as the peak systolic pressure and the trough diastolic pressure, typically 120 and 80 mm of mercury, respectively. The heart maintains these perfusion pressures by pumping 2 to 3 ounces of blood per contraction, approximately 72 times per minute. Thus, the heart pumps over 500,000 gallons of blood per year, and will beat over two and a half billion times in a lifetime.
Ventricular contraction
Unidirectional flow of blood through the heart is maintained by flexible valves at the entrance and exit points of both ventricles. As the valve leaflets snap closed they produce an audible sound which can be heard with a stethoscope, or even an ear pressed against the chest wall. The cardiac entrance valves (mitral on the left and tricuspid on the right) close at the beginning of ventricular contraction to prevent blood from being expelled backward into the venous system and produce the first heart sound. Likewise, the cardiac exit valves (aortic on the left and pulmonary on the right) are open during ventricular contraction to allow blood to flow into the arteries, but snap shut as the ventricles relax to prevent reverseCardiovascular irregularities
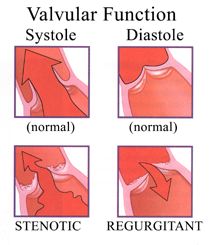 flow of arterial blood into the heart, and produce the second heart sound. Closure of the cardiac valves thus produces the "lub-dub....lub-dub...." sounds one hears when listening to the heart. Under normal circumstances blood flow through the heart, valves and vessels is smooth and silent because there is no turbulence. However, when the cardiac valves malfunction, either by leaking (a condition termed regurgitation) or by not fully opening (termed stenosis), turbulent blood flowing across the diseased valve produces a rushing sound or "heart murmer" by which a Cardiologist can frequently diagnose a particular valvular condition. Valvular disease may be congenital, such as being born with misshapen leaflets, or acquired such as rheumatic heart disease or bacterial and fungal valvular infections, termed infective endocarditis. Although the heart muscle can adapt to the extra work demands imposed by valvular regurgitation or stenosis by increasing the amount of heart muscle (cardiac hypertrophy), over many years this compensatory process is ultimately overwhelmed and the heart abnormally dilates and fails. Therefore, severe valvular disease generally requires surgical replacement with a mechanical or biological prosthesis to prevent the development of heart failure.
flow of arterial blood into the heart, and produce the second heart sound. Closure of the cardiac valves thus produces the "lub-dub....lub-dub...." sounds one hears when listening to the heart. Under normal circumstances blood flow through the heart, valves and vessels is smooth and silent because there is no turbulence. However, when the cardiac valves malfunction, either by leaking (a condition termed regurgitation) or by not fully opening (termed stenosis), turbulent blood flowing across the diseased valve produces a rushing sound or "heart murmer" by which a Cardiologist can frequently diagnose a particular valvular condition. Valvular disease may be congenital, such as being born with misshapen leaflets, or acquired such as rheumatic heart disease or bacterial and fungal valvular infections, termed infective endocarditis. Although the heart muscle can adapt to the extra work demands imposed by valvular regurgitation or stenosis by increasing the amount of heart muscle (cardiac hypertrophy), over many years this compensatory process is ultimately overwhelmed and the heart abnormally dilates and fails. Therefore, severe valvular disease generally requires surgical replacement with a mechanical or biological prosthesis to prevent the development of heart failure.
Electrocardiography
Cardiac muscleThe functional unit of the heart is the cardiac muscle cell or cardiomyocyte. Each cardiomyocyte maintains an electrical charge or potential across its cell membrane, and contracts when this potential is discharged. In order for all of the cardiomyocytes to contract at the same time and thus produce an effective muscular contraction, the heart also maintains its own electrical conducting system which coordinates the electrical activity of the heart.
The sum total of the simultaneous electrical discharging and re-charging of all the cardiomyocytes in the heart is sufficient to be detected by sensing probes placed on the exterior of the body at various positions around the heart. This is the principle behind the electrocardiograph or ECG which can be used to monitor the rhythm of the heart.
Also, since injured cardiomyocytes such as those suffering from lack of oxygen during a heart attack leak electrical current rather than discharge it in a coordinated manner, the altered electrical signal of the injured heart results in a characteristic ECG pattern which can lead to the diagnosis of acute myocardial infarction.
In contrast, dead cardiomyocytes or scarred cardiac muscle does not carry or maintain an electrical charge, and this absence of electrical activity is also detectable by ECG. Thus, a previously unrecognized or "silent" heart attack can be diagnosed by electrocardiogram, and even localized to a particular area of the heart by using multiple sensing probes or ECG leads.
Echocardiography
Whereas the electrical activity of the heart provides a powerful indicator of cardiac function and health, it is frequently desirable to directly monitor cardiac mechanical activity, that is the muscular contractions and relaxations. Technological advances over the past ten to twenty years have provided a variety of sophisticated methods to achieve this without injury, or even significant discomfort to patients. The most powerful diagnostic tool is echocardiography or "cardiac ultrasound", in which high frequency sound waves sufficiently intense to penetrate bodily tissues are directed into the chest and the pattern of reflected sound provides a real time image of the contracting heart and its component structures. Echocardiography can provide accurate measurements of heart chamber size and shape, contractile function, and the status of the four heart valves. Furthermore, by using the related technique of Doppler echocardiography the Cardiologist can directly visualize blood flow through the heart, and therefore identify regurgitant or stenosed valves by reversed or highly turbulent blood flow, respectively.Fluoroscopic cardiography
Cardiac function can also be assessed non-invasively by imaging a radioactively labeled blood pool within the cardiac ventricles during contraction and relaxation. This is the most accurate method for measuring cardiac contractile function because it is easy to precisely quantify the amount of radiation in the ventricle when it is most full and most nearly empty. The percent of blood expelled during each contraction, termed the ejection fraction, can then be mathematically calculated from these values; the typical ejection fraction of the left ventricle is 50 to 70% at rest, but can increase to 90% with strenuous exercise.Cardiac catheterisation
The oldest method of objectively evaluating cardiac function is still regarded by many as the "gold standard", the cardiac catheterization. During this procedure plastic tubes or catheters are harmlessly placed via arm or leg vessels into specific cardiac chambers or into the openings of arteries that feed the cardiac muscle, termed coronary arteries. Blood pressure and oxygen content can be measured at distinct points in the heart or great vessels to diagnose heart failure or to detect abnormal communications between cardiac structures. Dye is injected into the coronary arteries for visualization by X-ray motion pictures to detect arteriosclerotic blockages which may cause cardiac pain (angina) or lead to heart attacks. A cardiac catheterization procedure is also used to therapeutically restore coronary blood flow by balloon angioplasty or stenting of blocked arteries.Ohm's Law and the heart
Since the heart, arteries and veins comprise in integrated cardiovascular system, problems in the conduit vessels can obviously impact the function of the heart. As noted above, coronary arteriosclerosis, or cholesterol blocked arteries in the heart muscle, can injure the heart muscle by failing to provide necessary oxygen and nutrients to the cardiac muscle. When blood flow is completely and acutely blocked, typically by formation of a blood clot in a coronary artery, the heart muscle dies (a heart attack). A chronic subtotal blockage may not actually kill the heart muscle because some hypertension increases the work required to circulate blood to the vital organs such as the brain, kidneys and even the heart itself. Interestingly, this relationship between cardiac function and blood pressure is precisely described by an electrical equation, Ohm's law (E=IR), which states that the pressure gradient across a circuit (potential or E) is equal to the product of flow through the circuit (current or I) and the resistance in the circuit (R). Increased blood pressure (E) therefore must occur as a result of increased resistance in the arteries (R), assuming that the heart continues to pump the same volume of blood per minute (I). In fact, this is known to be the case and hypertension is routinely treated with vasodilator drugs which increase the size of arteries, decrease vascular resistance, and protect the heart.Hypertrophy
A critically important feature of cardiac muscle is that, like the brain, it has no capacity to regenerate. Shortly after birth the number of cardiomyocytes in a heart stabilizes and further growth of the heart can only occur by enlargement of existing cells, or hypertrophy. As noted previously, hypertrophy in response to valvular disease or increased blood pressure has limited ability to compensate for the increased work needed in these conditions, and ultimately fails. However, the type of cardiac hypertrophy which develops as a consequence of athletic training is purely beneficial, and even protective against heart failure. Therefore, in addition to risk factor modification for coronary atherosclerosis, such as not smoking and observing a low fat and cholesterol diet, aerobic physical training is an important preventative measure for heart disease, and a vital part of the therapeutic regime during cardiac rehabilitation. An exciting area of medical investigation in the cardiovascular field is the attempt to develop methods of regenerating cardiac muscle, or to modify the hypertrophic response to more resemble athletic hypertrophy, perhaps using gene transfer technology.